Growing thicker hair on your scalp is genuinely possible for most people, but it requires understanding what is actually driving your thinning before reaching for any product. The right starting point is a combination of honest self-assessment, basic blood work to rule out correctable deficiencies, a consistent scalp-and-root care routine, and targeted topical actives where appropriate. For a practical, step-by-step approach, see how to grow thicker hair from roots. None of this happens fast, visible improvement typically takes four to six months at minimum, but the evidence-based steps in this guide give you the best realistic shot at meaningful density gains.
How to Grow Thick Hair on Scalp: Evidence-Based Plan & Routine

Marcus Holloway
13 Jul 2026
Who this guide is for and how to use it
This guide is written for men and women of any age or hair type who are dealing with scalp thinning, visible hair loss, or simply want to build thicker, fuller hair from the roots up. It covers crown and top-of-scalp thinning, diffuse thinning across the whole head, post-shedding regrowth, and general density improvement. If you have curly hair or are dealing with traction-related thinning, there are sections aimed specifically at you.
The guide is structured to move you from understanding to action. Start with the biology and causes sections so you know what you are working with, then move into self-assessment and testing before committing to a routine. The topical actives and treatment sections build on that foundation. If you are already partway through this process and just need a specific piece, each section stands on its own.
How hair thickness and the growth cycle actually work
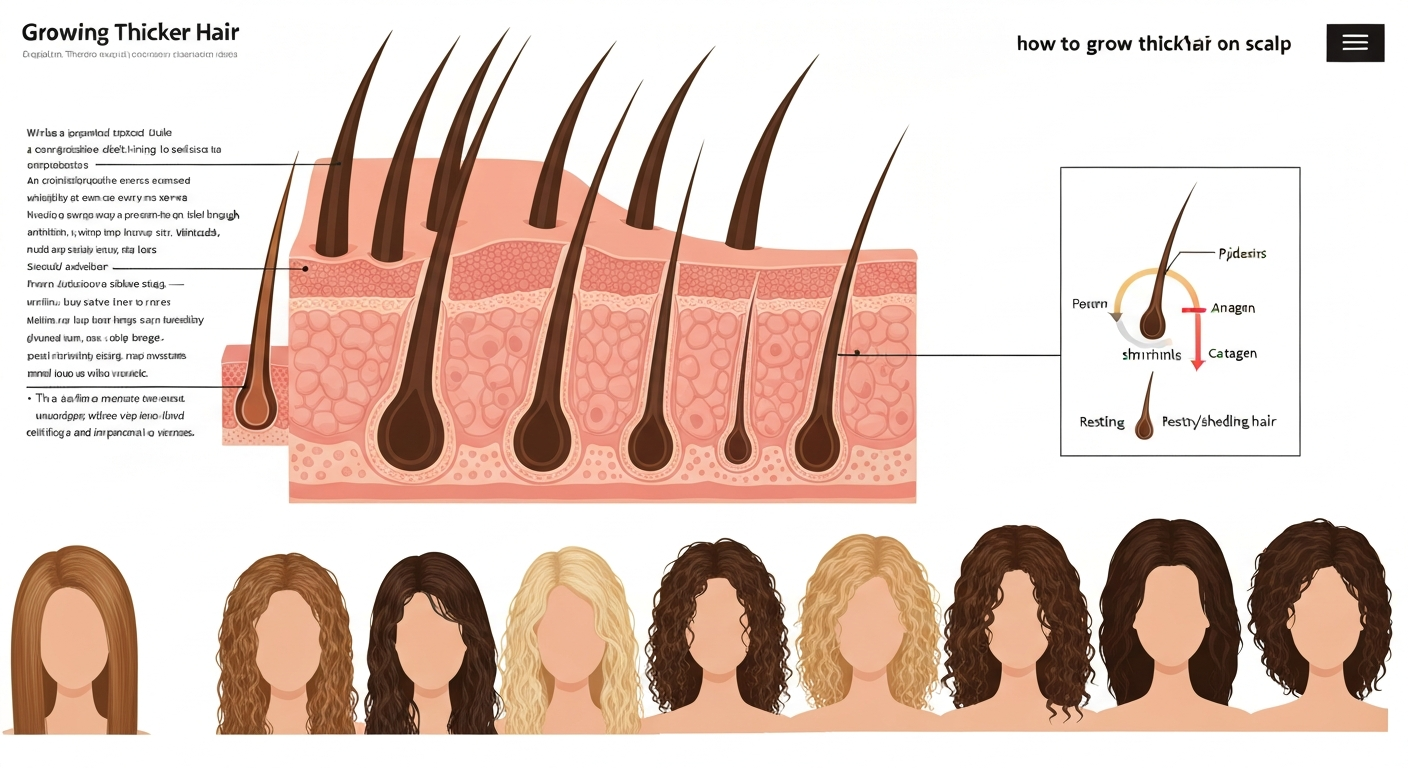
Each hair on your scalp grows from a follicle, a small, tube-like structure in the dermis that is fed by a tiny blood supply and packed with specialized cells. The diameter of the hair shaft that emerges from that follicle is what we experience as thickness, and it is largely determined by the size of the follicle itself. Bigger follicle, thicker strand. When we talk about growing thicker hair, we are really talking about either preserving follicle size, restoring miniaturized follicles back toward their original size, or optimizing the conditions that keep each follicle producing the fullest strand it can.
The hair growth cycle has three main phases. Anagen is the active growth phase, lasting roughly two to seven years on the scalp. The longer a hair stays in anagen, the longer and thicker it can grow. Catagen is a brief two-to-three week transition phase where the follicle shrinks. Telogen is the resting phase, lasting about three months, after which the old hair sheds and a new anagen hair begins. At any moment, roughly 85 to 90 percent of your scalp hairs are in anagen and about 10 to 15 percent are in telogen. When something disrupts this balance, illness, hormonal shifts, nutritional deficiency, chronic stress, more hairs than usual shift into telogen simultaneously, causing the diffuse shedding known as telogen effluvium.
Follicle miniaturization is the process behind pattern thinning. Androgens (particularly DHT, dihydrotestosterone) bind to receptors in genetically susceptible follicles and progressively shrink them over successive cycles. Each new hair that grows back is slightly finer and shorter than the last. Over years, the follicle may produce only a wispy vellus hair instead of the thick terminal hair it once did. The key insight here is that miniaturized follicles are not dead, they can often still respond to treatment, especially when caught early.
Common causes of scalp thinning, and why the pattern matters
Thinning can come from several completely different directions, and distinguishing between them is the most important step you will take. Treating a nutritional deficiency with minoxidil, for example, misses the actual problem. Here are the main causes worth knowing about.
- Androgenetic alopecia (AGA): The most common cause in both men and women. Driven by genetics and androgens, it produces predictable patterns — recession at the temples and crown thinning in men (Hamilton-Norwood scale), diffuse thinning at the part with crown predominance in women (Ludwig scale). Early-onset and family history are strong indicators.
- Hormonal shifts: Postpartum shedding (usually peaks 3–4 months after delivery and self-resolves within a year), perimenopause and menopause-related thinning, thyroid dysfunction (both hypo- and hyperthyroidism), polycystic ovary syndrome (PCOS), and elevated androgens from any cause can all trigger or worsen hair loss.
- Nutritional deficiencies: Iron deficiency (particularly low ferritin) is a well-documented and correctable driver of diffuse shedding. Deficiencies in zinc, vitamin D, vitamin B12, and protein intake can each contribute. Crash diets and very low-calorie periods are a reliable trigger.
- Traction alopecia: Persistent mechanical tension from tight braids, ponytails, locs, weaves, or extensions damages the follicle over time, starting at the hairline and temples. Caught early, it is reversible. Left unchecked, the damage can become permanent.
- Inflammatory and autoimmune conditions: Alopecia areata produces patchy, sharply demarcated round or oval bald patches. Scarring alopecias (lichen planopilaris, frontal fibrosing alopecia, central centrifugal cicatricial alopecia or CCCA) permanently destroy follicles and require urgent specialist referral. Seborrheic dermatitis and scalp psoriasis create inflammation that can worsen shedding without causing primary hair loss themselves.
- Medications and medical conditions: Chemotherapy, anticoagulants, retinoids, beta-blockers, and certain antidepressants are known to cause shedding. Chronic illness, significant surgery, and prolonged high stress also push hair into telogen effluvium.
- Chronic telogen effluvium: A persistent, diffuse daily shedding of more than 100–150 hairs per day that lasts beyond six months. Often has a stacking cause (multiple triggers simultaneously) and can be frustratingly hard to pin to one thing.
How to assess your own thinning
Before you spend any money on products or treatments, take thirty minutes to honestly document what is happening. This baseline matters more than you might think, because hair change is slow and memory is unreliable. Here is a practical self-assessment process you can do at home.
The part-width and crown check
Stand under a bright light (natural daylight or a ring light works well) and part your hair down the centre from forehead to crown. Take a photo directly from above. In healthy, dense hair the scalp should be barely visible. A clearly widened part, visible scalp at the crown, or a diffuse see-through quality at the top suggests reduced density. Repeat this photo in the same lighting and styling conditions every three months. It sounds tedious, but it is the single most reliable way to track whether things are improving, holding, or progressing.
The 60-second hair pull test
Loosely gather about 60 hairs between your thumb and first two fingers. Gently but firmly slide your fingers from root to tip with a light pulling tension. Fewer than six hairs in your hand is considered normal. More than six suggests active shedding and is worth noting. Do this on freshly washed, dry hair (to avoid counting shed hairs that are still being held in by styling products).
Daily shed count
If you are concerned about shedding volume, collect every hair you shed in one day, from the shower drain, brush, and pillow, and count them. 50 to 100 per day is within the normal range. Consistently over 150 per day, especially for more than a few weeks, is worth flagging to a clinician. Check whether hairs have a white bulb (telogen root) at the base, which confirms they have shed from the follicle naturally rather than breaking mid-shaft.
When to document and when to act
Take your baseline photos now, even if you are just starting to notice something. Set a three-month reminder to repeat them. If you notice itching, burning, tenderness, or sudden patchy loss, see a dermatologist sooner rather than later, those are signs that warrant faster evaluation. For gradual, diffuse thinning without scalp symptoms, a structured three-month monitoring period with the checks above is entirely reasonable before your first medical appointment.
Blood tests and medical checks worth getting
A large portion of hair thinning is driven by something correctable in your bloodwork. In my experience working through this with my own hair, getting tested first saved me from chasing treatments for a problem I did not actually have. The American Academy of Dermatology recommends evaluating hair loss with a targeted history and relevant blood tests before assuming a diagnosis.
Ask your GP or primary care clinician for the following panel when you present with hair thinning. You do not need to see a specialist first for initial testing, your family doctor can run most of these.
| Test | Why it matters | Key threshold to discuss |
|---|---|---|
| Ferritin (serum iron stores) | Low ferritin is one of the most common correctable causes of diffuse shedding — even when haemoglobin is normal | Many dermatologists suggest optimizing ferritin above 70 ng/mL for hair health, though lab normals vary |
| Full blood count (CBC) | Identifies anaemia and other blood abnormalities that affect hair cycling | Any values outside normal range should be investigated |
| Thyroid function: TSH, free T3, free T4 | Both hypothyroidism and hyperthyroidism reliably cause diffuse shedding | TSH above 4.0 or below 0.4 mIU/L warrants further investigation |
| Vitamin D (25-OH) | Deficiency linked to telogen effluvium and alopecia areata in observational studies | Below 50 nmol/L is commonly considered deficient; supplement accordingly |
| Vitamin B12 | Deficiency causes shedding, especially in vegetarians, vegans, or those on metformin | Below 200 pg/mL is low; supplementation and investigation of cause needed |
| Zinc | Deficiency accelerates shedding; commonly low in restricted diets | Low-normal or below-normal serum zinc warrants supplementation and dietary review |
| Androgens: DHEAS, free and total testosterone (women) | Elevated androgens signal PCOS or another hormonal driver of female pattern loss | Interpret in context of menstrual history and clinical symptoms |
| Sex hormone binding globulin (SHBG) | Low SHBG increases free androgen activity even when total testosterone is normal | Discuss in context of full hormone panel |
| HbA1c or fasting glucose (if indicated) | Insulin resistance and type 2 diabetes are associated with androgenetic alopecia | Standard diagnostic thresholds apply |
If your clinician suspects scarring alopecia, diagnostic uncertainty exists after initial tests, or you have a rapidly progressing or patchy pattern, the BAD and AAD both recommend referral to a dermatologist or trichologist, where a scalp biopsy can definitively guide treatment. Scarring alopecias like lichen planopilaris, frontal fibrosing alopecia, and CCCA require early specialist intervention, the window for preserving follicles is limited, and self-treatment is not appropriate.
Your daily scalp and hair care routine
Consistency in your daily routine builds the foundation that makes everything else, topical actives, supplements, treatments, more effective. The goal of your routine is a clean, mildly stimulated scalp with well-nourished strands that experience minimal breakage. Think of it less as a hair routine and more as a scalp care routine that happens to benefit your hair.
How often to wash and what to use
One of the most persistent myths is that washing your hair too often causes thinning. It does not. In fact, a clean scalp supports healthier follicular function. For most scalp types, washing every one to three days is appropriate. If you have a dry scalp or coarser, curly hair, two to three times per week is often ideal. If you are applying minoxidil or any leave-on topical active, you need a clean scalp for proper absorption, so do not skip washes to avoid washing out product, time your topical application after washing instead.
Choose a shampoo with a mild surfactant base (look for sodium lauryl sulfate-free or sulfate-free options if you experience scalp dryness or irritation). For those with seborrheic dermatitis or scalp inflammation, which worsens shedding, a shampoo containing 1 to 2 percent ketoconazole or 1 percent zinc pyrithione used two to three times per week provides both antifungal and mild anti-androgenic benefit at the scalp. Follow with a conditioner applied mid-shaft to ends only, not on the scalp itself, to avoid clogging follicular openings.
Morning routine: step by step
- Wash scalp on your scheduled wash day with a gentle or medicated shampoo, massaging the scalp (not the hair) for 60 seconds before rinsing.
- Apply conditioner from mid-shaft to ends. Rinse thoroughly. Gently pat — do not rub — hair dry with a microfibre towel or a soft cotton t-shirt.
- On wash days, apply your topical active (minoxidil or peptide serum) directly to the dry or slightly damp scalp at the crown and thinning areas. Use the applicator tip or dropper to part hair in sections so product reaches the scalp, not just the hair.
- Allow the topical to absorb for at least 30 to 60 minutes before styling. Minoxidil especially needs contact time with the scalp to work.
- Apply a lightweight leave-in conditioner or detangling spray to mid-lengths and ends if needed. Keep roots free of heavy product.
- Style with minimal heat. If you use heat tools, apply a heat protectant first and keep temperatures below 180°C (356°F) for fine or thinning hair.
Evening routine: step by step
- On non-wash evenings, apply your second topical active dose (if using twice-daily minoxidil solution) or skip application if using once-daily 5% foam.
- Perform a scalp massage for 4 to 5 minutes before bed — described in detail in the next section.
- Sleep on a satin or silk pillowcase to reduce friction-related breakage, which is especially relevant for curly, coily, or fine hair types.
- Loosely braid or tie hair with a soft fabric scrunchie if it is long enough to tangle. Avoid tight elastics at the crown or hairline where miniaturization is most active.
Scalp massage: how to do it in a way that actually helps
Scalp massage is one of those interventions that sounds almost too simple to work, but there is a reasonable mechanistic rationale behind it and some supporting clinical data. Mechanical stimulation increases local blood flow, which delivers more oxygen and nutrients to follicles. There is also evidence from small Japanese trials that standardized daily scalp massage over 24 weeks increased hair thickness measurably compared to baseline. It is not a miracle, but done consistently it costs you nothing and amplifies the benefit of any topical you apply immediately after.
Technique
Use the pads of your fingertips, not your nails. Place all ten fingers on the scalp and apply firm, circular pressure, moving in small circles rather than sliding across the hair. Work systematically: start at the base of the skull and hairline, move toward the sides (temporal regions), then work across the crown and top of the scalp. Pay particular attention to the areas where you have noticed thinning. Keep the pressure firm but comfortable, you should feel the scalp moving under your fingers, not just the hair sliding around.
Duration and schedule
Aim for at least four minutes per session, once or twice daily. Daily consistency over months matters far more than occasional longer sessions. If you are applying a topical serum or oil during the massage, use just enough to provide slip without flooding the scalp, excessive product leaves residue. If you are massaging as part of your pre-shampoo routine, a few drops of a carrier oil (jojoba, argan) work well. If massaging on a clean scalp before a topical active, do the massage first, then apply the active to a slightly stimulated scalp for improved absorption.
Tools
Manual fingertip massage is perfectly effective. Silicone scalp massager tools (available for a few dollars) add a mild additional mechanical stimulus and are easy to use in the shower. Vibrating electric scalp massagers exist and are fine if you find them motivating, but the evidence base for any specific tool over manual massage is not strong. The most important variable is doing it at all, regularly.
Topical actives: what the evidence actually shows and how to choose
This is where a lot of people get overwhelmed by options. The market is full of products making impressive claims, but only a handful of ingredients have robust clinical evidence behind them for growing thicker scalp hair. Here is an honest breakdown of what works, what shows early promise, and how to combine things safely.
Minoxidil: still the most evidence-backed topical option
Topical minoxidil remains the single most evidence-supported over-the-counter topical for growing thicker hair on the scalp. A Cochrane review found that both 2% and 5% topical minoxidil are significantly more effective than placebo for female pattern hair loss. In men, phase III randomized trials confirmed that 5% solution produces meaningfully larger hair-count increases than 2% or placebo. For women, the 5% foam formulation once daily has been shown in phase III trials to be at least as effective as 2% solution twice daily, with better tolerability and lower irritation. Phase III randomized trials in women showed that once‑daily 5% minoxidil foam provided non‑inferior or superior hair‑count outcomes compared with twice‑daily 2% solution, with lower irritancy and better cosmetic acceptability, with efficacy measurable by about 16–24 weeks and recommended assessment at 6–12 months.
How does it work? Minoxidil is a potassium channel opener that prolongs the anagen (growth) phase of the hair cycle and increases follicular blood flow. It does not block DHT, so it addresses the symptom (follicle miniaturization) rather than the hormonal driver. This is why it needs to be used continuously, stopping reverses gains within three to six months. A systematic review and meta-analysis of minoxidil trials confirmed that microscopic changes begin around three months, visible improvement often appears at four to six months, and peak measurable benefit takes nine to twelve months.
Practical notes: apply to a dry or slightly damp scalp, not to wet hair. Part the hair in sections at the crown and thinning areas so the dropper or applicator makes direct scalp contact. Wash hands thoroughly afterwards. Adverse effects documented in trials include local scalp irritation, contact dermatitis (more common with propylene glycol-containing solutions, which is why foam is often better tolerated), and in a minority of users, unwanted fine hair growth on the face or body. The Cochrane review 'Interventions for female pattern hair loss, Cochrane Review' summarizes common adverse effects of topical minoxidil as local scalp irritation, contact dermatitis (often linked to propylene glycol), and unwanted hypertrichosis, with systemic hypotension being rare blank" rel="noopener noreferrer">Interventions for female pattern hair loss — Cochrane Review. Systemic hypotension from topical application is rare but worth knowing about.
Ketoconazole shampoo: a useful supporting player
Ketoconazole at 1 to 2 percent concentration has a dual role: antifungal activity that reduces scalp inflammation from seborrheic dermatitis, plus a mild anti-androgenic effect at the scalp level. Studies comparing ketoconazole shampoo to minoxidil in mild AGA have shown comparable hair-density improvements, though the evidence base is smaller. Use it as a medicated shampoo two to three times per week rather than daily, leaving it on for two to three minutes before rinsing, and it works well alongside minoxidil without negative interactions.
Peptides and growth factor serums: promising, not yet gold standard
Copper peptides (GHK-Cu) and other bio-stimulating peptides have shown interesting results in some smaller trials, mechanisms include stimulating follicular stem cell activity, increasing vascularization, and extending anagen. Biomimetic peptides (for example, acetyl tetrapeptide-3 or redensyl-containing formulas) are showing up in increasingly well-designed clinical studies. The evidence is growing but not yet as robust as the minoxidil data. That said, peptide serums are generally well-tolerated, non-hormonal, and can reasonably be layered with minoxidil, apply the peptide serum first on clean scalp, allow to absorb, then apply minoxidil on top.
Ingredient checklist at a glance
| Ingredient | Concentration to look for | Evidence level | How to use | Key cautions |
|---|---|---|---|---|
| Minoxidil (topical) | 5% foam (once daily) or 2–5% solution (twice daily) | Strong — multiple RCTs, Cochrane review, systematic meta-analysis | Applied directly to scalp at thinning areas; continuous use required | Irritation, hypertrichosis (face/body), propylene glycol sensitivity in solutions; avoid contact with eyes |
| Ketoconazole | 1–2% shampoo | Moderate — comparative and observational studies | Medicated shampoo 2–3x/week, leave on 2–3 min before rinsing | Not for long-term daily use; mild interaction risk minimal at topical use |
| Zinc pyrithione | 1% shampoo | Moderate for seborrheic dermatitis; indirect hair benefit | Shampoo 2–3x/week | Generally well-tolerated; do not ingest |
| Copper peptides (GHK-Cu) | Varies — typically 1–5% in serums | Emerging — smaller trials, mechanistic data promising | Apply to clean scalp before or instead of minoxidil | Well-tolerated; few documented adverse effects at cosmetic concentrations |
| Acetyl tetrapeptide-3 / Redensyl | As per product formulation | Growing — branded clinical studies; independent RCT data limited | Apply as directed; can layer under minoxidil | Minimal known adverse effects; effectiveness varies by formulation |
| Topical finasteride (prescription) | 0.25% solution or spray — prescription only | Strong for men — phase III RCT vs placebo; lower systemic exposure than oral | Applied to scalp once daily; prescription required in most countries | Teratogenic risk — keep away from pregnant women; sexual adverse effects possible even topically |
| Saw palmetto (topical) | Varies | Limited — small studies, weaker than finasteride | Used in some OTC serums; can try as adjunct | Low risk topically; evidence base modest |
How to combine products safely
Keep it simple to start. Begin with one active, minoxidil, and run it for at least three months before adding anything else. This lets you identify what is working and what might be causing irritation. If you then want to add a peptide serum, apply it first to clean scalp, let it absorb for five minutes, then layer minoxidil on top. Ketoconazole shampoo is compatible with all topical actives because it rinses off. Do not apply minoxidil to irritated, broken, or sunburned scalp. If you develop contact dermatitis (redness, itching, flaking disproportionate to your baseline), stop the most recently added product for two weeks to isolate the cause.
Nutrition and supplements that support hair thickness
Hair is among the least metabolically essential tissues in the body, which means it is one of the first to suffer when your nutrition is suboptimal. Your follicles need an adequate supply of protein (hair is mostly keratin), iron, zinc, B vitamins, and vitamin D to cycle correctly and produce full-diameter shafts. There is no single supplement that dramatically thickens hair in the absence of a deficiency, but correcting a deficiency can make a noticeable difference within three to six months.
- Protein: Aim for at least 1.2 to 1.6 grams per kilogram of body weight per day from whole food sources. Hair is approximately 95% keratin (a protein), and inadequate intake is a direct limiting factor for production.
- Iron and ferritin: Many dermatologists suggest targeting ferritin above 70 ng/mL for hair health specifically, even though clinical lab normals are lower. If your ferritin comes back at 12 or 20, supplement with iron under clinician guidance and retest in three months.
- Vitamin D: A common deficiency linked to telogen effluvium and alopecia areata. Most adults in northern latitudes are insufficient by winter. Supplementing 1,000 to 2,000 IU daily is a reasonable starting point pending your lab results.
- Zinc: Supports keratin synthesis and follicle cell division. Found in red meat, pumpkin seeds, and legumes. Supplementing 25 mg elemental zinc daily is reasonable if dietary intake is low, but avoid high-dose supplementation long-term without a tested deficiency.
- Biotin: Only reliably useful if you have a genuine biotin deficiency (rare in most diets). It will not thicken hair in people with adequate intake, despite aggressive marketing.
- Omega-3 fatty acids: Some evidence from small studies that fish oil supplementation reduces hair shedding and improves perceived density. Safe, well-tolerated, and worth including at 1 to 2 g EPA/DHA daily.
- Saw palmetto (oral): A mild 5-alpha reductase inhibitor with a smaller evidence base than finasteride. Reasonable to try for mild AGA in men who prefer a non-prescription option, but do not expect finasteride-level results.
At-home and clinical treatments beyond topical actives
Once you have the daily routine and topicals established, there are additional tools that can meaningfully complement your approach, some at home, some requiring a clinician.
Microneedling (dermarolling)
Microneedling involves rolling a device studded with tiny needles across the scalp to create micro-injuries that trigger a wound-healing response, stimulate growth factors, and enhance absorption of topical actives applied afterward. A systematic review and meta-analysis found that combined microneedling plus minoxidil produced significantly better hair-count outcomes than minoxidil alone. Home dermarollers used for the scalp typically have needle lengths of 0.5 mm. Deeper lengths (1.0 to 1.5 mm) tend to be used in clinical settings. Use a sterile device weekly or biweekly, allow the scalp to settle for 24 hours before applying minoxidil, and do not use on an inflamed, infected, or actively irritated scalp.
Low-level laser therapy (LLLT)
Several devices using red light wavelengths of 630 to 660 nm, HairMax, Capillus, and similar FDA-cleared products, have been evaluated in randomized, sham-controlled trials. Results consistently show modest but statistically significant increases in terminal hair counts compared to sham. These devices are used for 10 to 20 minutes per session, several times per week. LLLT is best viewed as an adjunct to minoxidil or other primary treatments rather than a standalone solution. It is safe, non-invasive, and particularly useful for people who cannot tolerate topical actives well.
Prescription oral treatments
Oral finasteride at 1 mg/day is FDA-approved for men with androgenetic alopecia and has the strongest long-term evidence base of any systemic treatment. Randomized trials with five-year extension studies show sustained hair-count increases at the vertex and slowing of progression. Finasteride works by blocking the conversion of testosterone to DHT. Known adverse effects from product labeling and trials include decreased libido, erectile dysfunction, and ejaculation disorders in a minority of men, with reports of persistence after discontinuation. Finasteride is contraindicated in women of childbearing potential due to teratogenic risk to a male fetus.
For women, oral and topical finasteride are being studied in growing numbers of trials. Low-dose oral minoxidil (LDOM) at 0.5 to 2.5 mg/day has an expanding evidence base for both men and women with androgenetic alopecia and chronic telogen effluvium. A systematic review with meta-regression found dose-dependent efficacy, higher doses produced larger density gains but also more hypertrichosis and dose-related cardiovascular adverse events. Baseline blood pressure monitoring and a review of cardiac history are standard before starting LDOM. Spironolactone (50 to 200 mg/day) is used off-label in women, particularly those with signs of hyperandrogenism, and requires monitoring of electrolytes and blood pressure.
Platelet-rich plasma (PRP) and hair transplants
PRP involves drawing your own blood, concentrating the platelet-rich portion, and injecting it into the scalp to deliver growth factors directly to the follicular environment. Evidence quality is improving, multiple randomized trials show benefit over saline controls, but standardization of protocols varies widely between clinics, which makes results inconsistent. PRP is best considered for people who have already tried and sustained topical treatments for 12 months with incomplete results, or as a complement to medical therapy. Hair transplant surgery (follicular unit extraction or FUE) is a long-term option for those with stable pattern loss and adequate donor density, but it requires medical treatment to be maintained afterward to prevent continued loss of non-transplanted hairs.
Targeted strategies for special cases
Curly and coily hair types
If you have type 3 or type 4 (curly, coily) hair, the mechanics of hair care interact with thinning in some specific ways. The natural curl pattern makes it harder for sebum to travel down the shaft, so moisture retention and breakage prevention are high priorities. Wash every one to two weeks using a sulfate-free, hydrating shampoo or co-wash. Deep condition weekly to maintain elasticity and reduce mechanical breakage at the crown (where tension from styling is often highest). When growing thicker curly hair specifically, the focus on reducing breakage and protective styling is as important as any active treatment, a hair shaft that constantly breaks never builds visible length or density. For specific step-by-step advice, see our guide on how to grow thicker curly hair.
Crown and top-of-scalp thinning
The crown is the area most commonly affected by androgenetic thinning in both men and women. When applying minoxidil or any topical active, use the parting technique, divide hair into four to six sections across the crown and apply along each parting line so product touches scalp, not just hair. Volume-building styling products (root lifters, volumizing mousse) applied at the root before drying can provide immediate visual density while treatments work long-term. For practical styling tips on how to make thick hair grow down and lie flatter at the crown while you wait for density improvements, see our dedicated section on growth-down techniques. Avoid heavy oils or serums at the root, they flatten the hair and make thinning more visible.
Traction alopecia and hairline thinning
If your thinning is concentrated at the temples, edges, or nape and correlates with tight styling, the single most important intervention is removing the tension, immediately and permanently for those areas. Minoxidil applied to the affected areas can support regrowth if follicle damage has not yet progressed to scarring. Switch to protective styles that exert zero tension at the hairline, use soft fabric edges on wigs and caps, and avoid braiding directly on fragile edges.
Realistic timelines and when to see a specialist
The hardest part of this entire process is patience. Hair grows roughly 1 to 1.5 cm per month. Follicle miniaturization reverses slowly, and regrowth from a telogen effluvium shed takes a full cycle, typically three to six months after the trigger resolves. Here is what to realistically expect at each stage.
| Timeframe | What you might notice | What to do |
|---|---|---|
| 0–4 weeks | Possibly increased shedding if starting minoxidil (normal — hairs shift from telogen to anagen) | Stay consistent; this is expected and temporary |
| 1–3 months | Microscopic improvements in follicle activity; no visible change yet for most people | Continue routine; take comparison photos monthly |
| 3–6 months | Some people begin to notice less shedding, shorter baby hairs at the hairline, or slight improvement in part-width appearance | Compare photos; note whether shedding volume is decreasing |
| 6–12 months | Measurable visible improvement for people responding to treatment; fuller appearance at crown and roots | Reassess: if no change at all by 9–12 months, seek specialist review |
| 12+ months | Peak response for most topical and medical therapies; ongoing maintenance required to preserve gains | Continue treatment; do not stop based on success — stopping reverses gains |
Seek specialist evaluation from a dermatologist or trichologist without delay if you notice: rapidly spreading patches of complete hair loss, scalp burning, tenderness, persistent itching, or unusual scarring; complete lack of any response to consistent topical treatment after 9 to 12 months; hair loss that is accelerating despite treatment; any loss at eyebrows, eyelashes, or body hair alongside scalp thinning; or if you are a woman with signs of hyperandrogenism (irregular periods, acne, unexpected facial hair growth) alongside hair loss.
Growing thicker hair from the scalp is a long game that rewards consistency over intensity. The most effective approach combines honest diagnosis, correcting any nutritional deficiencies, a simple daily scalp care routine, appropriate topical actives applied correctly, and patience measured in months rather than weeks. The tools are there, what makes the difference is sticking with them long enough to let them work.
FAQ
What causes hair to appear thin on the scalp, and how does hair thickness/growth work?
Scalp hair thickness depends on hair shaft diameter, number of terminal follicles per area (density), and the hair growth cycle (anagen=growth, catagen=transition, telogen=rest/shedding). Common non‑scarring causes of thinning include androgenetic (pattern) hair loss, chronic telogen effluvium, nutritional or endocrine deficits (iron deficiency, thyroid disease), medication‑related loss, and traction/chemical damage. Scarring alopecias permanently destroy follicles and need early diagnosis. Treatable causes and phase shifts (shorter anagen, more follicles in telogen) explain why density falls and why therapies aim to lengthen anagen, increase follicle size, or prevent miniaturization.
What simple daily scalp-and-hair routine helps increase density at the roots and crown?
Daily/regular routine: 1) Cleanse 1–3× weekly (or more if oily) with a gentle sulfate‑free shampoo to keep follicles clear; 2) Use a lightweight conditioner on mid‑lengths and ends, avoid heavy product on the scalp; 3) Apply topical actives (e.g., minoxidil) to the thinning areas as prescribed; 4) Perform a 1–5 minute scalp massage or mechanical stimulation during washing or daily—moderate pressure to boost circulation and product absorption; 5) Limit heat, chemical processing, tight styles, and traction to reduce damage; 6) Sleep on a soft silk/cotton pillowcase and avoid repeated friction. Consistency matters: expect at least 3–6 months before visible change with conservative measures.
How should I choose and use topical minoxidil safely and effectively?
Topical minoxidil is first‑line, evidence‑based for androgenetic and many non‑scarring thinning patterns. Use 5% foam once daily or 5%/2% solution per product guidance (5% often more effective). Apply to a dry scalp at the crown/vertex and areas of thinning; allow to dry before styling. Expect microscopic changes by ~3 months and visible improvement by ~4–6 months; assess at 6–12 months. Common side effects: local irritation, contact dermatitis, and occasional facial hypertrichosis. Stopping reverses benefits within months. If irritation occurs, try foam, lower frequency, or discuss alternatives with a clinician.
When should I consider oral (systemic) treatments like finasteride or low‑dose oral minoxidil?
Consider systemic therapy when topical care and reversible causes have been addressed and thinning is progressive or bothersome. In men, oral finasteride 1 mg/day is effective for vertex/pattern hair loss but is contraindicated in women of childbearing potential due to teratogenicity and has possible sexual side effects. Low‑dose oral minoxidil (commonly 0.25–2.5 mg/day) can be effective for various non‑scarring alopecias but carries dose‑related risks (hypertrichosis, blood‑pressure effects) and requires baseline cardiac history and monitoring. Decisions should be made with a clinician after review of risks, contraception needs (for women), and monitoring plans.
What clinical procedures show evidence for improving scalp hair thickness?
Procedures with supportive evidence: 1) Microneedling combined with topical minoxidil—RCTs/meta‑analyses show superior hair counts vs minoxidil alone; 2) Platelet‑rich plasma (PRP)—multiple small trials suggest benefit for some patients but protocols vary; 3) Low‑level laser therapy (LLLT)/photobiomodulation—randomized sham‑controlled trials show modest increases in terminal hairs using home devices; 4) Hair transplantation—effective for permanent, localized restoration when donor hair is adequate. Efficacy, cost, number of sessions, and suitability vary; consult a dermatologist/trichologist for individualized planning.
Which blood tests and medical evaluations should I get to rule out treatable causes?
Essential baseline tests when thinning is new, sudden, or unexplained: thyroid function (TSH ± free T4), ferritin (iron stores), complete blood count (CBC), and in appropriate contexts, vitamin D, fasting glucose/HbA1c, and sex hormones (testosterone, SHBG, free androgen index) for signs of hyperandrogenism. For women of childbearing potential or when medication causes are suspected, review medications and pregnancy status. Refer to dermatology for suspected scarring alopecia or diagnostic uncertainty—scalp biopsy may be needed.
Next Articles

How to Grow Thicker Hair From Roots: A Step-by-Step Plan
Step-by-step plan to grow thicker hair from the roots by fixing shedding, scalp issues, nutrition, and safe topicals.

How to Grow Thicker Curly Hair: Routine for Length
Step-by-step routine to grow thicker curly hair: stop breakage, boost curl definition, support scalp health, and retain

How to Grow Hair Back Thicker: Step-by-Step Plan
Step-by-step plan to regrow thicker hair: scalp routine, nutrition, topical options, lifestyle fixes, and when to see a