Growing hair on your head comes down to three things: keeping your existing follicles healthy and active, removing whatever is slowing them down, and giving your body the raw materials it needs to actually build hair. You probably can't create brand-new follicles (more on that below), but most people have far more dormant or miniaturized follicles than they realize, and a consistent 12–24 week routine can wake a lot of them up. Start with your scalp, your diet, and a proven topical treatment, and you'll have a real shot at visible improvement. If you want a practical roadmap, follow the steps in this guide to grow more head hair over 12, 24 weeks.
How to Grow Hair on Head: Step-by-Step Follicle Plan

Marcus Holloway
7 Jun 2026

How hair growth actually works (and what 'new hair' really means)
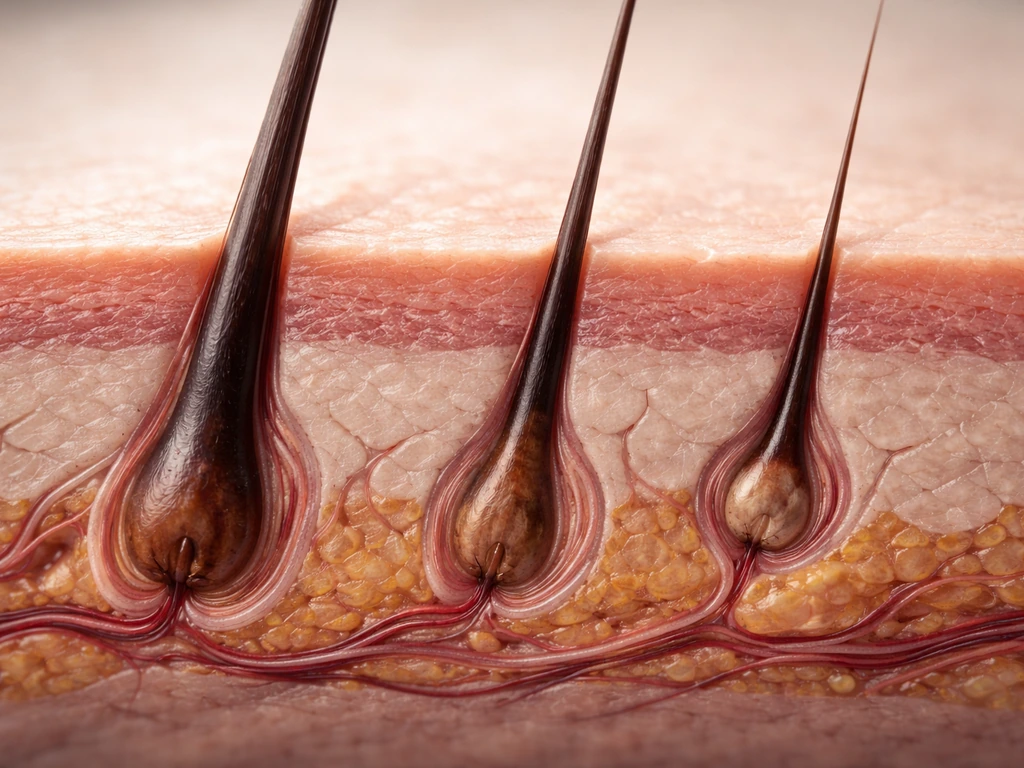
Every strand of hair grows from a follicle, a tiny organ embedded in your scalp. Each follicle runs on a repeating cycle: anagen (active growth), catagen (a brief transition), and telogen (resting). During anagen, cells at the base of the follicle divide rapidly and push a new hair shaft upward. Anagen lasts roughly 3–5 years on the scalp, which is why your hair can get quite long before it falls out.
Catagen takes just 2–3 weeks. Telogen lasts about 2–4 months, after which the old hair sheds and a new anagen cycle begins. At any given moment, around 84% of your scalp hairs are in anagen, with only 10–15% resting in telogen. That means the vast majority of your follicles are already working.
Here's the important distinction: 'growing new hair' almost never means creating brand-new follicles. You're born with all the follicles you'll ever have. What you're actually trying to do is either reactivate follicles that have gone dormant, or reverse miniaturization, a process where follicles shrink and produce progressively thinner, shorter hairs until they're barely visible. Miniaturization is the hallmark of pattern hair loss (androgenetic alopecia). When people describe regrowing hair with minoxidil or other treatments, what's happening is the follicle is being pushed back into anagen and the miniaturized hair is getting thicker and longer again, not new follicles being built from scratch.
The one exception is scarring (cicatricial) alopecia, where inflammation physically destroys the follicle structure. JAMA Dermatology notes that primary cicatricial (scarring) alopecias are inflammatory disorders that permanently destroy hair follicles and cause irreversible hair loss, making early diagnosis and intervention critical to preserve remaining viable follicles blank" rel="noopener noreferrer">scarring (cicatricial) alopecia, where inflammation physically destroys the follicle structure.. Once a follicle is destroyed by scarring, regrowth there isn't possible. Everything else, including androgenetic alopecia, telogen effluvium, traction damage, and nutrition-related shedding, involves follicles that are still structurally present and potentially recoverable. On examination, scarring alopecia is distinguished from non-scarring alopecia by blank" rel="noopener noreferrer">the absence versus presence of follicular openings, respectively.
Why you're losing or thinning hair in the first place
You need to have at least a working theory about your cause before you start, because the right approach differs depending on what's driving your hair loss. The good news is that most causes are non-scarring, meaning your follicles are still there waiting.
The most common culprits

- Androgenetic alopecia (pattern hair loss): Driven by genetics and androgens (primarily DHT), this causes gradual follicle miniaturization. In men it tends to show up at the temples and crown; in women it typically shows as central or crown thinning. It's the most common cause of hair loss overall.
- Telogen effluvium: A stress response where a large number of hairs are prematurely pushed into the resting (telogen) phase at once. You'll notice heavy shedding, usually 2–3 months after a trigger like illness, major surgery, crash dieting, childbirth, or prolonged emotional stress. It's usually self-limiting and resolves within 2–6 months once the trigger is gone.
- Nutritional deficiencies: Iron deficiency (especially low ferritin) and vitamin D deficiency are the most commonly linked to hair shedding. Zinc deficiency has also been associated with telogen effluvium. Severe protein deficiency can contribute, though this is rare if you eat a reasonably balanced diet.
- Thyroid disorders: Both hypothyroidism and hyperthyroidism can cause diffuse shedding. If your hair loss is diffuse and accompanied by fatigue, weight changes, or temperature sensitivity, get your TSH tested.
- Scalp conditions: Seborrheic dermatitis (dandruff) and fungal infections create an inflammatory environment that can impair follicle function. Traction from tight hairstyles can cause traction alopecia, which can become permanent if the pulling continues long enough.
- Scarring alopecia: Much rarer, but important to catch early. If you see redness, pustules, or areas with no visible follicular openings at all, see a dermatologist quickly. Early intervention can preserve the follicles that haven't been destroyed yet.
If your shedding is sudden and diffuse (all over, not patterned), a basic blood panel, complete blood count, TSH, ferritin, and vitamin D, is a reasonable first step. Your doctor can order these, and they're worth doing before spending money on supplements or treatments.
Build a scalp care routine that actually supports your follicles
Your scalp is skin, and it needs care. Clogged follicles, chronic inflammation, and a disrupted microbiome all interfere with healthy hair cycling. A good scalp routine isn't complicated, but it does need to be consistent.
Shampooing and scalp cleansing

Wash your scalp regularly enough to keep it clear of sebum buildup and dead skin, but not so aggressively that you strip it. For most people, every 2–3 days works well. If you have dandruff or seborrheic dermatitis, which is more common than people realize and is a real barrier to healthy follicle function, use an antifungal shampoo.
Ketoconazole 2% shampoo has the best clinical evidence: studies show it significantly reduces scaling, redness, and itching at 4 weeks compared to placebo, and it outperforms zinc pyrithione 1% for more severe cases. Use it 2–3 times per week until symptoms are controlled, then drop to once or twice a week as maintenance. Zinc pyrithione and selenium sulfide shampoos are solid alternatives if you want something over the counter for mild dandruff.
Scalp massage
Scalp massage is one of the easiest, lowest-cost things you can add to your routine. Spend 4–5 minutes massaging your scalp with your fingertips (not nails) daily, either during a shower or before applying a topical treatment. It increases blood circulation to the follicles and may mechanically stimulate the dermal papilla cells that drive hair growth. Use slow, firm, circular motions and cover the whole scalp, not just the areas of concern. You can also use a soft silicone scalp massager if that feels easier to sustain.
What to avoid on your scalp
- Tight hairstyles that put sustained tension on follicles, especially at the hairline and temples
- Excessive heat styling, which damages the hair shaft and, with repeated mechanical pulling, can stress follicles over time
- Leaving conditioner or heavy product buildup on the scalp itself (apply conditioner mid-shaft to ends)
- Picking, scratching, or aggressively rubbing a wet scalp with a towel
What to eat (and what to supplement) for hair growth
Hair is made mostly of keratin, a protein, and your follicles are among the most metabolically active cells in your body. They're sensitive to nutritional shortfalls, but they're also one of the first things your body deprioritizes when resources are scarce. That means deficiencies can slow growth noticeably, but if you're already eating well, adding more of a nutrient you're not deficient in rarely produces dramatic results.
Protein

Aim for adequate protein daily, roughly 0.7–1g per pound of body weight if you're active. Good sources include eggs, chicken, fish, legumes, Greek yogurt, and tofu. Unless you're severely restricting calories or eating a very limited diet, outright protein deficiency is unlikely, but getting enough is still a foundation of the plan.
Iron and ferritin
Low ferritin (stored iron) is one of the more commonly overlooked contributors to hair shedding, particularly in women. If your blood test shows low ferritin, work on correcting it through food (red meat, lentils, spinach with vitamin C to aid absorption) or a supplement under your doctor's guidance. Don't supplement iron if your levels are normal, excess iron has its own risks.
Vitamin D
Vitamin D deficiency has been linked to both androgenetic alopecia and telogen effluvium in multiple reviews, and it's extremely common, especially in people who spend most of their time indoors. Get your level tested. If you're deficient, a supplement (typically 1,000–2,000 IU daily, or more if your doctor recommends) makes sense. You'll also get some from fatty fish, egg yolks, and fortified foods.
Zinc and other micronutrients
Zinc deficiency has been associated with telogen effluvium. You can get zinc from meat, shellfish (oysters especially), pumpkin seeds, and legumes. If your diet is varied and includes these foods, you're likely fine. Biotin is frequently marketed for hair, but the evidence only really supports it if you have an actual biotin deficiency, which is rare. If you're eating eggs, nuts, and whole grains, your biotin intake is almost certainly adequate. The overall supplement evidence base for hair is mixed and heterogeneous, so targeted supplementation based on your actual deficiencies beats buying generic 'hair growth' formulas.
| Nutrient | What it does for hair | Best food sources | Supplement if deficient? |
|---|---|---|---|
| Protein | Builds keratin and hair structure | Eggs, chicken, fish, legumes, Greek yogurt | Rarely needed; focus on diet |
| Iron / Ferritin | Fuels rapidly dividing follicle cells | Red meat, lentils, spinach, fortified cereals | Yes, if ferritin is low |
| Vitamin D | Supports follicle cycling and immune regulation | Fatty fish, egg yolks, sunlight | Yes, if blood level is low |
| Zinc | Protein synthesis and follicle repair | Oysters, pumpkin seeds, meat, legumes | Yes, if deficient |
| Biotin | Keratin infrastructure | Eggs, nuts, whole grains | Only if genuinely deficient |
Topical treatments: what actually works and how to use them
Minoxidil: still the gold standard

Minoxidil is the most evidence-backed over-the-counter topical treatment for hair regrowth. It works by prolonging the anagen phase and increasing blood flow to the follicle. The 5% formulation (foam or solution) is available without a prescription for men; women typically start with 2% though 5% is increasingly used under medical guidance. Apply it directly to a dry scalp twice daily (or once daily for the foam version).
Part your hair to expose the scalp in thinning areas, apply, and don't wash your hair for at least 4 hours after. One important thing to know: you may see increased shedding in the first 2–4 weeks. This is normal. It means follicles are cycling, not that the treatment is failing.
Give it a full 4 months before deciding it isn't working. If you stop using it, any regrowth typically reverses within 3–4 months, so you need to commit to ongoing use.
Microneedling as an add-on
Microneedling with a dermaroller (0.5–1.5mm needle length for the scalp) has shown promise as an adjunct to minoxidil. A randomized controlled study found the combination of microneedling plus minoxidil produced significantly greater hair count increases than minoxidil alone. The proposed mechanism is that microneedling creates micro-wounds that trigger growth factor release and also improves minoxidil penetration into the scalp. If you use a dermaroller, do it once a week on the thinning areas before applying minoxidil, sterilize it properly, and be gentle. This is worth considering if you've been on minoxidil for 3+ months with limited results.
Rosemary oil
A well-cited randomized trial compared rosemary oil to minoxidil 2% over 6 months and found both groups had significant increases in hair count at the endpoint. Rosemary oil won't work as well as 5% minoxidil, but it's a reasonable option if you prefer a natural approach or want to use it alongside minoxidil. Mix a few drops of rosemary essential oil into a carrier oil (like jojoba or coconut), massage into the scalp, leave on for 30 minutes, and wash out. Do this 3–4 times a week.
Caffeine-based topicals
Caffeine applied topically may stimulate hair follicles by blocking the effects of DHT at the follicle level. An open-label noninferiority trial comparing a 0.2% caffeine-based solution to 5% minoxidil found no significant difference between the two in men with androgenetic alopecia, which is more promising than expected. Caffeine-based shampoos and serums are widely available and worth including in your routine, though they're probably better as a complement than a replacement for minoxidil.
Low-level laser therapy (LLLT)
LLLT devices (laser caps, combs, and helmets) have been evaluated in systematic reviews and meta-analyses for androgenetic alopecia, with some evidence of modest benefit. They're FDA-cleared for hair loss. The evidence is real but the effect size tends to be moderate, and quality devices are expensive. Think of LLLT as a potential add-on for people who want to maximize every angle, not a first-line standalone treatment.
The lifestyle factors that quietly sabotage your follicles
Sleep
Your body does its cellular repair work during sleep, and that includes follicle cycling. Chronic sleep deprivation elevates cortisol, which is a direct trigger for telogen effluvium. Aim for 7–9 hours consistently. If your sleep quality is poor, that's worth addressing separately, because no topical treatment will fully compensate for a chronically stressed nervous system.
Stress
Psychological stress is one of the documented triggers for telogen effluvium, where a large cohort of follicles simultaneously shift into the resting phase. The frustrating part is that the shedding typically shows up 2–3 months after the stressful period, so by the time you're losing hair, the trigger may already be in the past. Managing ongoing stress through exercise, sleep, and whatever sustainable practices work for you (breathwork, therapy, time outdoors) is genuinely part of a hair regrowth plan, not a soft add-on.
Smoking
Smoking impairs microcirculation, including blood flow to the scalp and follicles. It also generates oxidative stress that accelerates follicle aging. If you smoke, this is one more good reason to quit.
Styling habits
Tight ponytails, braids, and extensions that pull continuously on the follicle cause traction alopecia, which starts as inflammation and broken hairs but can progress to permanent scarring if the traction isn't relieved. If thinning is worse at the hairline or temples, look at your styling habits first. Switch to loose styles, avoid overnight tension, and give your scalp a break. This is especially relevant when growing out hair on the sides, crown, or top of the head, where different areas may respond to different styling pressures. If you want to grow crown hair specifically, use the same follicle-first approach and tailor it to your likely cause, timing, and scalp routine.
Your 12–24 week action plan
Here's how to put it all together in a realistic, trackable plan. Hair grows slowly (roughly half an inch per month at best), and treatments take time to shift the follicle cycle. The goal for the first 12 weeks is to build the routine, not to see full results. By weeks 16–24, you should be able to make a real assessment.
Weeks 1–4: assess, set the baseline, start the basics
- Get a blood test if you haven't already: CBC, TSH, ferritin, and vitamin D at minimum. Address any deficiencies that come back.
- Take clear photos of your scalp in the thinning areas under consistent lighting. Do this in the same spot, same light, same angle every 4 weeks. This is your only reliable tracking tool.
- Start a scalp care routine: wash every 2–3 days with a gentle (or antifungal if needed) shampoo. Add 4–5 minutes of daily scalp massage.
- Assess your diet. Are you eating enough protein, iron-rich foods, and vitamin D sources? Fill obvious gaps.
- Start minoxidil 5% (foam or solution) if you've decided to use it. Be prepared for the initial shedding phase and don't panic.
- Note any tight hairstyles or styling habits that could be causing tension and change them now.
Weeks 5–12: add adjuncts and build consistency
- If you're using minoxidil, keep going. The initial shed should settle down by weeks 4–6.
- Add rosemary oil massages 3–4 times per week if you want a natural complement.
- Consider introducing once-weekly microneedling before minoxidil application if your progress feels slow.
- Take your 8-week photos and compare to week 1. Look for reduced shedding, any new fine hairs, and overall density rather than dramatic length changes.
- Stay consistent on sleep (7–9 hours) and keep stress management active. These aren't optional background items.
Weeks 13–24: evaluate, adjust, and decide next steps
- At the 4-month mark, compare your photos critically. Minoxidil's label specifically states that if you see no results after 4 months, consult a doctor. If you're seeing improvement, keep going.
- If results are minimal, this is the time to see a dermatologist. They can use trichoscopy (a magnified scalp exam at roughly x20–x160) to distinguish between androgenetic alopecia, telogen effluvium, and scarring, and they can discuss prescription options like oral minoxidil or finasteride.
- If your telogen effluvium trigger has been resolved, expect to see meaningful regrowth between months 3 and 6. Most cases resolve within 6–8 months once the cause is gone.
- Keep taking monthly photos. Progress with hair is notoriously hard to perceive day-to-day. Photos over 3–6 months tell the real story.
- If you've addressed nutrition deficiencies, confirm improvement with a retest at 3–4 months.
How to tell if it's working
The first signs of progress are usually a reduction in shedding (fewer hairs in the drain, on your pillow, in your brush) and the appearance of short, fine new hairs in thinning areas. These hairs will be soft and lighter than your existing hair at first. They thicken over time as the follicle strengthens. Density and coverage improve more slowly than the initial regrowth, so expect to see noticeable texture improvement before you see full coverage.
If you're 24 weeks in with consistent effort and still seeing no response, get a proper diagnosis. Scarring alopecia, an untreated thyroid disorder, or a cause you haven't yet identified could be the reason, and those need targeted medical intervention rather than more of the same routine.
Depending on where your thinning is concentrated, the approach can be similar but slightly tailored. Thinning at the crown, on top of the head, or on the sides each involves the same follicle biology, but the patterns can signal different causes and respond somewhat differently to treatment.
Getting clarity on your specific pattern early helps you focus your efforts where they'll matter most, especially if your goal is how to grow hair on top of head on top of the head. If you're focused on the crown, use the same 12, 24 week routine, but pay extra attention to scalp health and consistent topical treatment in that area how to grow crown hair.
Getting clarity on your specific pattern early helps you focus your efforts where they'll matter most.
FAQ
How do I know if I’m dealing with miniaturization (pattern hair loss) versus a shedding problem like telogen effluvium?
A practical clue is the pattern and timing. Miniaturization usually shows gradual thinning in typical areas (often crown or temples) with shorter, finer hairs over months to years. Telogen effluvium often looks more sudden and diffuse, with increased shedding that starts about 2 to 3 months after a trigger (stress, illness, weight loss, new meds). If you see mostly shedding with relatively uniform density changes, focus first on identifying and correcting the trigger and labs, then layer in regrowth treatments if needed.
When should I stop “trialing” treatments and get a dermatologist evaluation?
If you have no meaningful change by around 24 weeks with consistent scalp care and a properly used topical option, get assessed. Earlier evaluation is smart if you have symptoms like burning, scalp tenderness, patchy scarring-looking lesions, or rapid progression, because those raise the possibility of scarring alopecia or another medical cause that needs targeted treatment.
Is it normal to shed more after starting minoxidil, and what if the shedding never calms down?
Initial shedding for 2 to 4 weeks can be a sign that follicles are moving into a new cycle, so don’t judge too early. If shedding continues aggressively beyond about 4 to 6 weeks, double-check you’re using the right dose, applying to a dry scalp consistently, and not worsening dandruff or irritation. Ongoing heavy shedding may also point to an underlying trigger that needs separate workup.
Can I use minoxidil if I have dandruff or sensitive skin?
Yes, but you should control scalp inflammation first because irritation can worsen shedding and make you stop the treatment. If you’re using ketoconazole (or another anti-dandruff shampoo), consider alternating application days so you’re not stripping the scalp while starting minoxidil. Also watch for stinging or redness after application, which may mean the product needs formulation adjustment or medical guidance.
What’s the biggest mistake people make with topical minoxidil?
Common failures are under-applying, applying to a scalp that isn’t exposed properly (hair blocks contact), or missing doses early and then trying to compensate later. Another big one is washing hair too soon after application. If you want reliable results, part the hair to reach the scalp and avoid washing for at least 4 hours after each application.
Does hair regrowth require taking supplements, even if my diet seems good?
Not automatically. Supplements work best when they target a confirmed deficiency, like low ferritin or vitamin D. If your labs are normal and your diet is reasonably varied, adding “hair” supplements often provides minimal benefit and can create avoidable side effects (for example, excess iron). Consider targeted supplementation only after testing or when your diet has a clear gap.
Can I grow hair faster by using higher-strength minoxidil or more often?
More is not always better. Higher frequency can increase irritation, which can undermine progress, and the plan already accounts for waiting long enough to judge results. If you want to change strength or schedule, do it deliberately and ideally with clinician guidance, especially if you’re female or prone to scalp sensitivity.
Will rosemary oil or caffeine replace minoxidil?
They can be add-ons, but they’re unlikely to match the effect size of 5% minoxidil for androgenetic alopecia. If you choose them, treat it as a complement and still monitor response over months. If you are not seeing early improvements in shedding or fine regrowth by the expected timeframe, consider stepping up to evidence-backed options rather than continuing indefinitely.
How should I microneedle safely, and what frequency is reasonable?
Stick to the thinning areas rather than the whole scalp, and keep it to about once per week. Use proper sterilization and gentle technique, avoid sessions if you have active dermatitis, sores, or significant irritation, and stop if you develop worsening redness or tenderness. If you’ve already used minoxidil for 3+ months with little progress, microneedling may be most useful as an adjunct.
Can LLLT (laser caps or combs) be used alongside topical treatments?
Yes, for many people it can be layered as an add-on rather than a replacement. The more important factor is device consistency (regular use as directed) because laser effects are typically modest. If you combine approaches, keep one variable at a time so you can tell whether you’re actually improving.
What hair growth expectations should I have if my goal is the top of my head or crown?
Even with the right routine, the first visible change is often texture and fine regrowth, not immediate density. Crown and top-of-head patterns can respond, but they often take the full 16 to 24 week window to assess because the follicles may already be miniaturized. Track photos and shedding counts weekly so you can distinguish progress from normal day-to-day variation.
Is traction from hairstyling something I can ignore while trying to regrow hair?
No. If traction alopecia is contributing, tightening or tension can keep inflammation going and can delay or permanently limit regrowth. Switch to looser styles, avoid pulling during sleep, and be extra cautious with edges, temples, and side areas while you’re attempting regrowth.
If I’m a smoker, will quitting make a measurable difference for hair regrowth?
Quitting is beneficial for scalp microcirculation and oxidative stress, and it removes a factor that can accelerate follicle aging. Hair outcomes won’t reverse overnight, but stopping smoking supports the overall environment your follicles need while other treatments are working over months.
Next Articles

How to Grow More Head Hair: Step-by-Step Guide
Step-by-step guide to grow more head hair with nutrition, topical care, lifestyle fixes, timelines, and when to see a de

How to Grow Crown Hair: Natural Steps and Evidence-Based Treatments
Learn how to grow crown hair with a plan: assess cause, improve scalp health, use natural tips, and add evidence-based t

Tips on How to Grow Your Hair Out: A Step by Step Guide
Step-by-step tips to grow hair out: stop breakage, build scalp routine, nutrition, safe actives, and track progress.